AI Prior Authorization Software: A Complete Guide for Small and Specialty Clinics
AI Prior Authorization Software: A Complete Guide for Small and Specialty Clinics AI Prior Authorization Software: A Complete Guide for Small and Specialty Clinics AI Prior Authorization Software is quickly becoming the difference between clinics that lose hours to paperwork and clinics that don’t. Every week, staff at small and specialty practices spend hours chasing documentation, filling payer forms, and following up on requests that vanish into a portal somewhere. Care gets delayed. Revenue gets delayed. Staff get burned out. This guide walks through what AI Prior Authorization Software actually does, how it fits into a real clinic workflow, and how to evaluate and roll one out without disrupting your practice. Why Prior Authorization Is Especially Painful for Small and Specialty Clinics A single prior authorization request can eat up an hour or more of staff time. Multiply that across dozens of weekly requests and the cost becomes obvious. Specialty clinics feel this harder than most. Radiology, orthopedics, cardiology, and oncology practices deal with higher PA volume and more complex documentation requirements than general primary care. Every payer has its own rules, portals, forms, and language for medical necessity. What satisfies one insurer will get flagged by another. This variability is where most of the real pain lives. It shows up as denials, resubmissions, rescheduled procedures, and patient no-shows tied directly to authorization delays. This guide covers what AI Prior Authorization Software is, what it automates, how to evaluate tools, and how to roll one out safely. Prior Authorization 101: A Quick, Practical Overview Prior authorization is the approval a payer requires before covering certain procedures. In specialty care, this shows up constantly around advanced imaging, injections, surgeries, specialty medications, and oncology regimens. The typical lifecycle looks like this: an order is placed, staff check the benefit and PA requirement, documentation is gathered, the request is submitted, someone follows up, and the payer approves or denies it. Denials often lead to appeals, which restart parts of this cycle. Most PA failures trace back to a handful of causes. Missing clinical notes, wrong codes, no proof of conservative therapy, mismatched diagnosis and procedure codes, and missed deadlines are the usual suspects. Doing prior authorization well is mostly about process discipline and matching documentation to what each payer actually wants. What AI Prior Authorization Software Actually Means Not every tool marketed this way does the same thing. Basic macros, form fillers, and clearinghouse-only tools automate small pieces of the process. True AI Prior Authorization Software goes further. It should detect which orders likely need authorization, assemble supporting documentation automatically, prepare payer-specific packets, guide staff through submission, and track status until resolution. The best systems use a human-in-the-loop model. The AI drafts and assembles the request. Staff reviews it and submits it. Be wary of vendors promising fully autonomous submissions everywhere or zero denials. Realistic AI Prior Authorization Software reduces workload and errors. It does not eliminate the need for human judgment. The 5 Tasks AI Can Reliably Automate in Prior Authorization Good AI Prior Authorization Software tends to focus on five specific tasks rather than trying to replace the entire process. Authorization detection flags orders likely to require PA based on payer and procedure patterns, which cuts down on last-minute surprises. Documentation collection pulls imaging reports, prior therapy notes, and labs into one organized packet. Request preparation generates payer-specific forms and medical necessity narratives with the correct codes attached. Submission assistance walks staff through portal or fax workflows so nothing gets left out. Tracking and follow-up keeps a live queue of pending requests and deadlines so nothing falls through the cracks. A radiology clinic might use this for MRI approvals. An orthopedic practice might use it for joint injections. Cardiology groups often lean on it for echo and CT authorizations, while oncology practices use it to manage regimen-heavy submissions. How AI Reduces Prior Authorization Denials Most denials come down to a small set of causes. Missing information, mismatched criteria, weak evidence of conservative therapy, and coding errors account for the majority of them. AI Prior Authorization Software helps by applying payer-specific checklists before submission. It scores completeness, flags gaps, and builds narratives mapped directly to medical necessity criteria. This creates a consistent packet structure regardless of which staff member handles the request. Consistency matters more than people expect. A lot of denial variance comes from different staff handling requests differently. Results still depend on accurate inputs, active review, and staying current with payer rule changes, which shift often. What to Look for in AI Prior Authorization Software Choosing the right platform matters as much as choosing to adopt one at all. A few things are worth checking closely before signing anything. Workflow fit comes first. Does the software match your existing order-to-submission process, or will your team need to rebuild how they work? Specialty support matters too, since imaging, procedures, and specialty medications each need different documentation logic. Payer coverage should include your top insurers and their preferred submission methods. Documentation intelligence should mean the tool understands which note sections actually matter, not just that it can attach a PDF. Security and compliance are non-negotiable. Look for HIPAA alignment, encryption, and audit logging. For a full breakdown of criteria clinics should weigh, this guide on choosing a healthcare AI automation platform for your clinic covers the details worth asking vendors about directly. Integration approach is another common sticking point. Some tools require deep EHR integration while others work alongside any system through upload or extraction. This resource on how EHR integration speeds up the prior authorization process explains what to expect either way. Build vs Buy vs Outsource Small and specialty clinics generally have three paths available, and each comes with real tradeoffs. Approach Best Fit Main Tradeoff Buy AI Prior Authorization Software Clinics with steady, recurring PA volume Requires vendor evaluation and setup time Outsource to a PA service Clinics needing overflow support occasionally Adds communication delays and depends on vendor quality Build custom automation Rarely worth it for small
How EHR Integration Speeds Up The Prior Authorization Process

How EHR Integration Speeds Up the Prior Authorization Process EHR Integration is quietly becoming the biggest lever specialty clinics have for cutting prior authorization delays. If you have ever watched a prior auth request sit in limbo for days while a patient waits for an MRI or a specialty medication, you already know the cost. The paperwork itself is not the real problem. The real problem is how many hands, systems, and re-typed fields a single request has to pass through before a payer even looks at it. This article breaks down why prior authorization feels so slow, what EHR Integration actually means in this context, and how it speeds up the process at almost every step. Why prior authorization feels slow (and where the time actually goes) Prior authorization, often shortened to PA, is a payer requirement before certain care can proceed. It typically applies to medications, imaging, procedures, and durable medical equipment. The typical PA timeline looks simple on paper. Clinical documentation gets gathered, payer rules get checked, forms get completed, requests get submitted, and then the back and forth begins. In reality, most of the delay hides inside that back and forth. Missing or incorrect data forces staff to dig through charts again. Fax machines and payer portals fragment the process even further. Every payer has different requirements, which means duplicate entry becomes the norm rather than the exception. Staff end up typing the same clinical details into three or four different systems. These delays are not just inconvenient. They push back patient care, drive clinician burnout, and quietly leak revenue through denials and rework. Anyone who has read about how AI can reduce physician burnout caused by administrative paperwork knows this cycle is well documented across specialties. This is exactly where EHR Integration earns its place. It reduces what many revenue cycle leaders call administrative latency, which is the lag between a clinical decision and the payer actually receiving what it needs. What EHR Integration means in a prior authorization workflow EHR Integration is often misunderstood as simply having two systems that can technically talk to each other. That is not enough on its own. Real EHR Integration means three things happening together. Data moves in both directions. The workflow itself is embedded inside the clinician and staff experience. Status visibility is available without logging into a separate portal. There are different levels of EHR Integration worth knowing. Basic integration allows attachments or exports between systems. Intermediate integration offers single sign on access to a payer or vendor portal. Advanced EHR Integration goes further. It embeds rules and automatically captures data directly inside the clinical workflow. Optimized integration closes the loop entirely and adds analytics on top. You may also hear terms like ePA, short for electronic prior authorization, or interoperability, which is a broader term than workflow integration. RPA, or robotic process automation, is not the same thing as true EHR Integration either. The goal behind all of this is simple. Reduce clicks, remove re-keying, ensure nothing is missing, and get payers a faster, cleaner response. How EHR Integration speeds up prior authorization Here are seven concrete ways EHR Integration shortens the prior authorization timeline. First, it auto-populates PA requests using existing patient data. Demographics, coverage details, NPI numbers, diagnosis codes, medication history, labs, and imaging results all pull in automatically. Second, it runs real-time eligibility and benefit checks. Staff can confirm coverage and whether a PA is even necessary before anyone submits anything. Third, payer rules surface directly inside the EHR. Medical policies, step therapy requirements, and quantity limits become visible before submission, not after a denial. Fourth, smart documentation prompts appear during the actual visit. Clinicians get reminded to capture failed therapies or contraindications while the information is fresh. Fifth, supporting documents attach in one click. Chart notes, labs, and imaging reports get labeled and formatted correctly the first time. Sixth, submission happens electronically from inside the EHR instead of through fax or phone. Immediate validation catches missing fields before they cause a delay. Seventh, closed-loop status updates land directly in the EHR task queue. Payer questions, approvals, and denials show up without a single portal login. The before and after workflow for staff, clinicians, and patients Before EHR Integration, a typical PA request means a staff member manually pulling the chart. They re-enter data into a payer portal, fax notes, and follow up by phone repeatedly. Clinicians get interrupted mid-day when criteria are missing. That interruption alone is a major driver of burnout across specialty practices. After EHR Integration, the request starts inside the EHR itself. Data captures automatically, a criteria checklist appears, and submission happens electronically without leaving the chart. Clinicians experience fewer interruptions. PA specialists spend less time on rework. Billing and revenue cycle teams see fewer denials, and patients start treatment sooner. Consider a specialty medication request as an example. Instead of a specialist calling the pharmacy and faxing lab values separately, the labs attach automatically and the request submits the same day. Clinics that have documented how specialty clinics can standardize prior authorization workflows across staff tend to see this exact shift once EHR Integration is in place. Key integration capabilities to look for Not every EHR Integration is built the same way. Some capabilities matter far more than others when speed is the goal. Look for in-workflow ePA initiation rather than a separate portal experience. Standards support matters too, specifically HL7 and FHIR for data exchange and NCPDP SCRIPT for medication-related ePA. Bi-directional, closed-loop communication with payer responses is essential. Without it, staff still have to check a portal manually for updates. A rules engine or clinical decision support at the point of ordering helps catch requirements early. Attachment automation and proper document mapping prevent formatting rejections. Tasking and queue management with an audit trail keeps everything organized across a team. Analytics on turnaround time, denial reasons, and payer performance help leadership spot patterns. Finally, ask about fallback paths. Not every payer supports ePA, so a
Electronic Prior Authorization vs. Manual Submission: A Practical Comparison

Electronic Prior Authorization vs. Manual Submission: A Practical Comparison Electronic prior authorization is no longer a nice-to-have upgrade for busy clinics — it is increasingly the line between a practice that schedules patients on time and one that hemorrhages revenue through rework, delays, and staff burnout. If you run prior auth for a specialty clinic, a radiology group, or a multi-provider practice, you already know the manual version of this process: a fax goes out, a phone call follows it, someone logs into a payer portal, and then you wait. This article walks through what separates electronic prior authorization (ePA) from manual submission across every dimension that actually matters to the people doing this work every day — speed, accuracy, visibility, cost, patient experience, and scale. Prior Authorization in Plain English Before comparing methods, it helps to be precise about what prior authorization actually is. It is a payer requirement that a provider obtain approval before a service, procedure, or drug will be covered. The payer wants to confirm medical necessity before committing to payment. What triggers a PA varies, but the common categories are high-cost imaging (MRI, CT, PET), specialty medications, durable medical equipment, elective surgical procedures, and advanced diagnostics. Once a PA is triggered, several parties are involved: the ordering provider, the administrative or billing staff who gather documentation, the payer’s utilization management (UM) team that reviews the request, and ultimately the patient whose care is waiting on the outcome. A successful prior authorization request means the right clinical documentation — ICD-10 and CPT codes, clinical notes, imaging results, prior treatment history — was submitted to the right payer in the right format, with approval in hand before the date of service. That last part is where most of the friction lives. Manual vs. Electronic: What Each One Actually Means Manual prior authorization means submitting through fax, phone calls, email attachments, or payer-specific web portals. It often involves copying and pasting patient and insurance data between systems, printing and scanning clinical documents, and tracking status through spreadsheets, sticky notes, or shared inboxes. Electronic prior authorization means submitting through a standardized electronic transaction — typically integrated into the EHR or RCM platform — with structured data fields, automated routing, and real-time or near-real-time status updates returned from the payer. A common misconception is worth addressing directly: logging into a payer portal and submitting a form is not ePA. True ePA involves structured data transactions, built-in validation, and system-to-system communication. The portal is just a more organized version of manual. Many organizations run a hybrid. Some payers support ePA; others still require fax. Some service lines are high enough volume to justify automation; others are not. The goal is not to eliminate all manual work — it is to reduce how much of it your team carries. A Side-by-Side Comparison That Actually Means Something Rather than a general overview, here is a breakdown across six dimensions that prior auth teams feel every day. Speed: Turnaround Time and Time-to-Schedule Manual PA is slow by design. A request goes out by fax, sits in a queue, requires a follow-up call, and if anything is missing, the whole cycle restarts. Many payers have business-hour-only review windows, which adds calendar days to a process already measured in days rather than hours. Prior authorization automation can cut approval times by up to 80%, which translates directly into fewer rescheduled appointments and less downstream billing friction. With ePA, the submission reaches the payer faster, with fewer touchpoints, and status updates come back through the same channel. It is still not always instant — complex cases still go to clinical review — but the administrative lag is dramatically shorter. What to track: median time from order to submission, submission to payer response, and approval to scheduled appointment date. Accuracy: Completeness, Coding, and Documentation Quality Manual submission introduces multiple failure points. Wrong form version, missing attachments, ICD-10/CPT misalignment, outdated medical necessity criteria — any of these sends a request back to square one. The rework is labor-intensive and delays care. ePA platforms have built-in validations. Required fields cannot be left blank. Code combinations are checked against payer rules before submission. That said, ePA cannot fix weak clinical documentation upstream. Clinical documentation quality is what makes or breaks insurance approvals — and that reality does not change regardless of which submission method you use. A practical fix for both methods: build specialty-specific checklists and documentation templates so that whoever is pulling the chart knows exactly what needs to be in the request before it goes anywhere. Visibility: Status Tracking, Accountability, and Audit Trail This is where manual PA falls apart most visibly. Status lives in whoever last touched the case. One staff member called the payer on Tuesday; another faxed an addendum on Thursday; no one updated the tracker. When a patient calls asking about their authorization, no one has a clean answer. ePA creates a timestamped, centralized record of every action — submission, payer acknowledgment, pending status, approval or denial. That audit trail matters for patient communication, for escalating pended cases, and for defending against payer disputes. It also matters internally for QA and for identifying which payers or service lines are causing recurring problems. Labor and Cost: Staff Time, Rework, and Burnout Manual PA is a staffing sink. The hidden cost of manual prior authorization in radiology practices — and across specialty medicine broadly — runs far deeper than the obvious salary line. Factor in overtime during volume spikes, the training burden of managing credentials across a dozen different payer portals, the opportunity cost of delayed scheduling, and the turnover that comes when staff spend their days chasing faxes and listening to hold music. Here is a rough framework for estimating your current cost: Cost Component What to Measure Typical Range Staff time per authorization Minutes per PA, all touches 20 to 45 minutes (manual) Rework rate % of PAs requiring resubmission 15% to 30% in manual workflows Denial rate linked to PA Claim denials traceable
Clinical Documentation 101: Why It Makes or Breaks Your Insurance Approvals
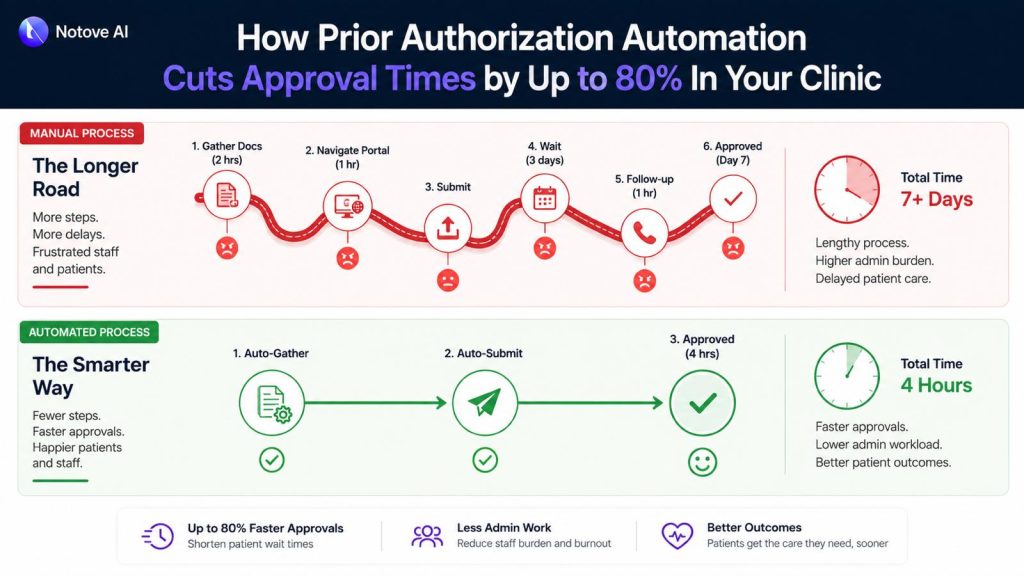
How Prior Authorization Automation Cuts Approval Times by Up to 80% In Your Clinic Prior authorization automation is no longer something only large hospital systems get to enjoy. It is quickly becoming the line between a clinic that runs on schedule and one that quietly loses hours, revenue, and staff bandwidth every single week. If your team spends significant chunks of the day pulling chart notes, calling payer lines, and hunting down status updates on requests submitted three days ago, you already understand the problem. What you may not yet see clearly is how much of that work does not actually require a human being to do it. Why Prior Authorizations Keep Slowing Clinics Down The average manual PA request moves through several predictable stages: confirming whether authorization is needed, gathering clinical documentation, completing payer-specific forms, submitting the request, and following up when no response arrives. In a busy specialty practice, that full cycle takes anywhere from 45 minutes to well over two hours per case. The deeper problem is variance. Each payer carries its own clinical criteria, its own portal workflow, its own definition of what counts as sufficient medical necessity evidence. Staff handling five different payers on the same afternoon are constantly switching gears, and that constant shifting is exactly where errors get introduced. A missing attachment, a mismatched code, or a letter that does not address the payer’s specific criteria sends the request back, and the clock resets. What is unfolding right now goes well beyond scheduling friction. The accumulation of these daily administrative loops is contributing to delayed care, staff overtime, and appointment cancellations that never show up on any dashboard but cost the clinic real revenue all the same. What Prior Authorization Automation Actually Means There is genuine confusion in the market about this term, so it is worth being precise. Prior authorization automation refers to software, typically AI-powered, that handles the repetitive non-clinical stages of the PA process: detecting when a procedure requires authorization, pulling the relevant clinical documentation, preparing the payer-specific request, and tracking submission status through to resolution. What it does not do is replace clinical judgment. The physician still owns the medical decision. The care team still determines what treatment is appropriate. Automation removes the administrative scaffolding that surrounds that decision and consumes time disproportionate to its actual clinical value. Basic automation relies on rules and static templates. A more capable AI agent goes further: it orchestrates the full workflow, extracts documentation intelligently from the EHR, drafts payer-specific letters, and surfaces any gaps before the request ever goes out. That distinction matters because the majority of denials are not rooted in the clinical decision itself. They trace back to gaps in how clinical documentation is prepared and presented, gaps that a well-designed system catches at the preparation stage rather than after a denial arrives. The Mechanics Behind an 80% Reduction in Approval Time The 80% figure is not a promise about payer response time. Payer turnaround is outside anyone’s control. The reduction comes from compressing the stages that are entirely within the clinic’s control: preparation, error correction, and follow-up. Here is a realistic look at where time actually goes in a manual PA workflow compared to an automated one: Stage Manual Time Automated Time Time Saved Authorization detection 10 to 15 minutes Under 1 minute ~93% Documentation assembly 20 to 30 minutes 3 to 5 minutes ~85% Form and letter preparation 15 to 20 minutes 2 to 4 minutes ~82% Staff review and submission 10 to 15 minutes 3 to 5 minutes ~67% Follow-up and status tracking 15 to 30 minutes 5 to 8 minutes ~70% Total per PA request 70 to 110 minutes 13 to 23 minutes ~79% The savings concentrate in two stages: documentation assembly and form preparation. These require digging through charts, interpreting payer-specific criteria, and reformatting clinical evidence into submission-ready packets. An AI system that understands those requirements and can surface the right evidence from an EHR handles that work in seconds. The 5-Step Workflow a Good System Should Handle When evaluating any prior authorization automation tool, use these five steps as your checklist. Each one maps to a common failure point in manual processing. Step 1 is authorization detection. The system should flag, at the point of order creation, that the procedure requires PA. This single step prevents the last-minute chaos of a procedure scheduled without authorization and the patient callbacks that follow. Step 2 is documentation assembly. This is the single biggest time sink in any manual process. A capable system pulls recent clinical notes, diagnoses, prior treatment history, imaging results, and lab values, then maps those findings to the specific payer’s medical necessity criteria. The hidden costs that manual documentation assembly creates in high-volume practices illustrate exactly how much time and revenue disappears when this stage runs on human effort alone. Step 3 is payer-specific request preparation. Every payer uses different forms, requires different fields, and favors different submission channels. Automation generates a payer-ready packet with correct formatting, proper attachments, and consistent structure, reducing the chance of a pend or return-to-provider before the request even gets reviewed. Step 4 is staff review and submission. This is where the human stays in the loop. A well-designed workflow displays the full request, the assembled documentation, and any open flags on a single screen. The authorization specialist reviews, edits if needed, and submits. Getting this stage under five minutes is the target. Step 5 is submission tracking and follow-up. This is where delays quietly accumulate in manual workflows with no one noticing until a scheduled procedure gets pulled. A good system maintains a live dashboard of every request status, captures payer notes, and sends automated reminders when follow-up windows open. Where Clinics See the Biggest Return The ROI from prior authorization automation shows up across several categories at once. The most visible is staff hours recovered each week. When each PA request takes 15 minutes instead of 90, a team managing 20 requests per week reclaims
Clinical Documentation 101: Why It Makes or Breaks Your Insurance Approvals

The Prior Authorization Crisis In 2026: 93% of Physicians Say It Delays Patient Care The Prior Authorization Crisis has quietly become one of the most damaging forces inside American healthcare, and by 2026, it is no longer just a billing complaint. It is a patient safety issue. Picture this: a cardiologist orders a stress test for a patient with chest pain. The patient is anxious, already canceling work to make the appointment. Three days pass. Then five. The insurer wants more documentation. Someone on the care team spends forty minutes on hold. The test slot disappears. A new one is scheduled two weeks out. The patient ends up in the emergency room first. That sequence, or something close to it, plays out in clinics across the country every single day. According to the American Medical Association, 93% of physicians report that prior authorization delays necessary patient care. That figure is not a talking point. It is a description of how the system actually moves, and what it costs people while it moves. What Prior Authorization Actually Is Prior authorization (PA) is a requirement from a health insurer that a provider get approval before a covered service, medication, or procedure will be reimbursed. The stated rationale is reasonable: manage costs, reduce unnecessary care, and ensure treatments meet evidence-based standards. Utilization management in theory is not a bad idea. In practice, the system has drifted far from that original purpose. Approval criteria are inconsistent across payers and plans. Documentation requirements are opaque and frequently change. Denials arrive without clear clinical justification. Providers submit, get asked for more information, request a peer-to-peer review, wait for a callback that may never come, get denied, appeal, and start over. Each step adds days. Sometimes weeks. And at every stage, the patient is waiting. What the Statistic Looks Like at the Bedside When 93% of physicians say prior authorization delays care, the translation into clinic life looks like this: a patient with a lump waits two weeks longer for imaging. A teenager in a mental health crisis waits days for a medication to get approved before it can be prescribed. A post-surgical patient in pain cannot start physical therapy because the authorization window closed while the paperwork was in transit. The delays hit hardest in cancer workups, cardiology evaluations, chronic pain management, behavioral health, and infusion therapies including biologics. These are not elective situations. Prolonged waits in these categories lead to condition progression, unplanned emergency visits, and in some cases, worse long-term outcomes that are entirely preventable. There is also a psychological cost that does not appear in claim data. Patients grow frustrated, lose confidence in their care team, and sometimes give up on treatment entirely. Clinicians experience a specific kind of moral injury when they know what a patient needs, the evidence supports it, and the insurer is the only barrier. Why It Got Worse by 2026 Five distinct pressures have converged to make the Prior Authorization Crisis worse in 2026 than it was even three years ago. More services and drugs are being routed through PA requirements. Payer lists have expanded, and step therapy protocols, which require patients to try and fail cheaper treatments before accessing what their physician actually prescribed, have become more common across specialties. Payer rule fragmentation has made the administrative load nearly unmanageable. Each insurer has different portals, different forms, different documentation requirements, and different turnaround timeframes. A practice dealing with fifteen payers is maintaining fifteen different sets of rules. Staffing shortages and burnout mean there are fewer people to chase approvals. High turnover increases the chance of errors, rework, and dropped follow-ups. EHR documentation and payer-required fields rarely match. Missing specific clinical language, sometimes called the “magic words” that trigger approval, causes automatic denials even when the clinical case is solid. Finally, “digital PA” tools that insurers have rolled out often do not save time. They still require manual attachments, ask the same questions in different formats, and ultimately route to a human review queue with no faster resolution. The Real Cost: Time, Money, and Clinical Distortion The cost of prior authorization goes beyond frustration. Cost Category What It Looks Like in Practice Clinician time Physicians and staff spend an average of 12+ hours per week on PA tasks across a small practice Delayed revenue Approved services billed weeks late; denied services rebilled at significant labor cost Appeal labor Each denial that goes to appeal adds 2 to 4 hours of staff time with uncertain outcomes Treatment abandonment 1 in 4 patients abandon treatment when PA delays exceed 2 weeks, per AMA data Clinical distortion Providers increasingly choose what is easiest to approve over what is clinically optimal That last row is the most corrosive. When the path of least resistance in clinical decision-making becomes “what will the insurer approve without a fight,” the system is no longer serving patients. It is serving paperwork. The equity dimension is also significant. Patients with less flexible work schedules, those with limited English proficiency, those without consistent coverage, and those unfamiliar with how to navigate insurance processes are far less likely to successfully advocate for themselves through a denial or delay. They are disproportionately the ones who fall out of care entirely. Where the Patient Journey Breaks Starting from a patient’s symptom and tracing the path forward, the failure points are predictable: the provider submits a PA request with incomplete documentation, or the clinical notes use language that does not match payer criteria. The insurer requests more information. The provider is in clinic and cannot respond immediately. The payer closes the window. A peer-to-peer review gets scheduled. This is a call between the ordering physician and a payer-employed medical reviewer to discuss the case. The problem is that payer-appointed reviewers often call during clinic hours and give narrow windows to respond. Physicians in back-to-back appointments miss the window. The denial stands. Meanwhile, the imaging slot the patient was supposed to fill gets taken. A new appointment requires a new authorization, and
Clinical Documentation 101: Why It Makes or Breaks Your Insurance Approvals

Clinical Documentation 101: Why It Makes or Breaks Your Insurance Approvals Clinical documentation is the difference between a claim that sails through and one that stalls for weeks while your patient sits in limbo. If you have worked in behavioral health or any specialty that deals with payer review, you already know this feeling: the care plan is solid, the clinical reasoning is there, the patient clearly needs this level of care, and yet the prior authorization or continued stay request comes back denied. Not because the care was wrong. Because the note did not prove it in the way a reviewer could act on it. This article covers documentation that supports insurance approvals: prior authorizations, continued stay reviews, claims, and audits. It is written for clinicians, care teams, and anyone involved in treatment planning, utilization review, or payer-facing documentation in behavioral health and healthcare operations. Nothing here is legal advice, and you should always follow your payer, state, and facility policies. What this is, is practical guidance on how to close the gap between clinical quality and payer sufficiency. What Insurers Actually Look for (And Why “Good Notes” Still Get Denied) Payers do not read your notes the way a clinical supervisor does. They are looking for coverage criteria, and they are looking fast. A compassionate narrative about a patient’s struggles is not the same thing as a defensible medical necessity argument, even if it tells a better story. Coverage decisions are evidence-based and criteria-driven. Reviewers are checking for a specific set of signals: diagnosis, severity, risk, functional impairment, skilled need, and treatment response. When any of those pieces are absent or vague, the decision defaults to denial. The most common disconnects that trigger denials are not clinical failures. They are documentation failures. A diagnosis that does not match the symptoms described in the assessment. Goals so broad they cannot be measured. No documented objective change between review periods. Risk documented on admission and then never mentioned again. A discharge plan that does not exist. These are the gaps that reviewers find, and they find them every time. Clinical Documentation 101: The Non-Negotiables Clinical documentation in this context is a legal record, a clinical record, and a reimbursement record all at once. Most payers expect to see the following components consistently across the chart: presenting problem, diagnosis support, risk, functional impact, treatment plan, skilled interventions, treatment response, ongoing need, and discharge or step-down planning. That last word, consistently, matters more than most teams realize. A thorough intake assessment means nothing if the daily progress notes describe a different patient. The assessment, the plan, the notes, the utilization review summaries, and the discharge summary all need to tell the same story with the same facts. Medical Necessity: How to Document It So a Reviewer Cannot Miss It Medical necessity answers three questions in plain language: why this level of care, why now, and why for this patient specifically. Reviewers are asking the same three questions in a slightly different form: Is the problem covered? Is the level of care appropriate? Is there evidence it is working and still needed? To answer those questions clearly, your documentation needs to include severity, acuity, risk, functional impairment, history of failed lower levels of care, why the current intensity or structure is required, and a clinical rationale tied to individualized goals. Not boilerplate. Not a template dropped in unchanged from the last patient. The clinical rationale needs to reflect this person’s presentation. Objective Evidence: Turning Symptoms Into Reviewable Proof Payers prefer observable, quantifiable detail over subjective clinical impressions. That does not mean your clinical judgment does not matter. It means your clinical judgment needs to be shown, not just stated. Objective documentation looks like this: frequency, duration, and intensity of symptoms; sleep and appetite changes; attendance and participation; functioning in daily activities, work, or school; withdrawal scales or vitals where applicable; and standardized measures when they are being used. Documenting a trend over time, from baseline to current status and the delta in between, tied directly to your interventions, is what builds a reviewable case for ongoing care. The phrase “doing well” without any metrics is one of the fastest ways to trigger a denial. Show what changed, and show what is still impaired. Risk and Safety: Document Like It Matters Risk documentation directly supports level-of-care decisions and continued stay justifications. What to include: suicidal and homicidal ideation, self-harm behaviors, psychosis or mania, intoxication or withdrawal risk, domestic violence or environmental safety concerns, and inability to adequately care for oneself. Beyond listing risks, document protective factors, assign a risk level with your rationale, and connect that risk level to the safety plan elements you have in place. One common pitfall that reviewers notice immediately: risk is documented thoroughly on day one and then disappears from the notes for a week. Continuity of risk documentation is not optional. It is what keeps a continued stay review from falling apart. Goals, Interventions, Response: The Care Loop That Drives Continued Stay The logic reviewers follow is a loop: problem leads to goal, goal leads to intervention, intervention leads to patient response, response leads to the next plan. If any link in that chain is broken or missing, the case for continued stay weakens. Goals need to be specific and measurable. “Reduce anxiety” is not a goal a reviewer can evaluate. “Patient will identify and use two coping strategies when anxiety exceeds a self-rated 7/10, three times per week” gives a reviewer something to look for. Document what the clinician actually did as a skilled intervention, not just that a session occurred. And capture the response: what is working, what is not, and what changed in the plan as a result. Where Approvals Fail Most Often: 8 Documentation Mistakes That Trigger Denials Mistake Why It Causes a Denial Vague language (“stable,” “improving”) with no evidence Reviewers cannot confirm necessity without measurable support Copy/paste notes that do not reflect today’s presentation Signals that the note does not represent
The Hidden Cost of Manual Prior Authorization in Radiology Practices
The Hidden Cost of Manual Prior Authorization in Radiology Practices Manual Prior Authorization is costing your radiology practice far more than you realize, and most of it never shows up as a single line item anywhere in your financials. It hides in payroll, in scanner downtime, in the patient who got tired of waiting and booked somewhere else, and in the authorization specialist who quietly started looking for a new job three months ago. This article breaks down where those costs actually live, how to find them in your own operation, and what you can do about it before they compound further. What “Manual Prior Authorization” Actually Looks Like in Radiology Before talking about costs, it helps to be specific about what manual prior authorization means in practice. It is not a single task. It is a chain of human-driven steps: verifying benefits and eligibility, gathering clinical documentation from the referring provider, looking up payer-specific criteria, submitting through a portal or by fax or by phone (sometimes all three for the same case), scheduling a peer-to-peer if the payer pushes back, checking status repeatedly, documenting the outcome, and finally releasing the appointment to scheduling. For advanced imaging, the chain gets longer. CT, MRI, and PET scans often go through radiology benefit managers like eviCore or NIA rather than directly to the payer. Each RBM has its own portal, its own clinical criteria, and its own timeline. A case that starts with a fax might end with a peer-to-peer call three days later. And if the clinical note from the ordering physician was incomplete when it arrived, the whole process stalls and restarts. The word “manual” matters because it means a person is doing each of those steps, across every case, every day, while the phone is also ringing and the portal is also timing out. The Hidden Costs: Where It Hits Your Practice 1. Direct Labor: The Authorization Shadow Workforce The most immediate cost is the staff time being consumed. Schedulers, PA specialists, clinical reviewers, billing staff, and occasionally radiologists for peer-to-peer calls are all part of the authorization ecosystem. Most practices have never added up what that actually costs. A simple framework: multiply your average minutes per case by your blended hourly rate across roles involved, then by your monthly authorization volume. Even at a conservative estimate of 20 minutes per case for routine submissions and a blended rate of $25 per hour, a practice processing 400 authorizations a month is spending around $3,300 in direct labor just on the submission step. Add status checks, rework, and peer-to-peer prep, and that number climbs fast. What compounds this is the interruption cost. Every time a staff member stops to log into a different portal, chase a missing clinical note, or wait on hold with an insurance company, they lose their working rhythm on everything else. 2. Revenue Delay: Slower Approvals, Slower Cash Authorization delay creates a chain reaction that goes straight to your cash flow. No approval means no scheduled scan. No scheduled scan means no charge capture. No charge capture means slower payment, and in the meantime the auth validity window is ticking down. Payer authorizations typically expire within 90 days, sometimes less. If a case gets approved but scheduling is delayed because of backlog or patient availability, that auth can expire before the scan ever happens. Now the team has to resubmit, restart the clock, and the scanner slot sits open in the meantime. High-deductible plan patients add another wrinkle. When timing is uncertain, the conversation about patient financial responsibility gets harder to have, and practices often defer it rather than deal with it mid-auth chaos. That deferred conversation becomes a collections problem later. 3. Denials and Rework: Doing the Work Twice Denial rates tied to authorization issues are not small. Common drivers include medical necessity criteria mismatch, incomplete clinical documentation, CPT and ICD-10 pairing errors, expired authorizations, and site-of-service problems. Each of those is a failure point that a manual workflow is more likely to produce than an assisted one. When a denial comes in, someone has to investigate the reason, gather additional documentation, coordinate a peer-to-peer if applicable, resubmit, and then follow up again. That is often 45 to 90 minutes of additional work on top of what was already spent. For a practice with a meaningful denial rate, this rework is effectively paying twice for the same case. 4. Capacity Loss: Empty Scanner Slots Nobody Can Fill Last-Minute Pending authorizations block schedule slots. When an approval comes through unexpectedly, there is rarely a patient ready to fill that slot on short notice. When an authorization falls through at the last minute, the patient gets rescheduled and the time is lost. The downstream effects reach the whole operation: longer wait times for routine cases, overtime for technologists when urgent add-ons get pushed in, and referring physician frustration when their patients can not get timely appointments. Radiology runs on throughput. Anything that creates irregular scheduling gaps undermines the efficiency the whole revenue model depends on. 5. Patient Leakage: Authorization Friction Sends Patients Elsewhere Patients are not loyal to imaging centers that are hard to schedule. If the authorization process creates repeated calls, unclear status updates, or last-minute cancellations, a meaningful share of patients will follow their referring physician’s next suggestion to a different facility. They often do not complain. They just do not come back. Referring offices feel this too. Their staff will gravitate toward imaging centers that give them clean, predictable authorization experiences. If your practice is the one that always needs to call back for more information or keeps cases in limbo for days, you will start losing referrals to competitors who have tightened up their intake process. 6. Compliance and Audit Exposure Manual authorization processes produce inconsistent documentation. An approval obtained by phone gets logged differently than one obtained through a portal. A fax confirmation gets filed somewhere that is not the same place as the portal screenshot. When an audit comes, or
How Medical Prior Authorization Delays Are Directly Harming Patient Outcomes
How Medical Prior Authorization Delays Are Directly Harming Patient Outcomes Medical Prior Authorization, the process insurers use to approve treatments before they are covered, has become one of the most debated friction points in American healthcare. And the debate is not really about whether the process should exist. It is about what happens in the time between a clinician ordering care and an insurer signing off on it. That gap is not neutral. It has a clinical cost, and in many cases, that cost is paid by the patient. This article looks at where delays actually occur, what they do to patient outcomes, and what can realistically be done about it across patients, practices, and payers. What Prior Authorization Actually Is (And How It Works in Practice) Prior authorization (PA) is a requirement that a clinician or facility obtain insurer approval before certain medications, procedures, imaging studies, or specialist visits will be covered. The intended logic is that it filters out low-value or unnecessary care and controls spending. The workflow typically looks like this: a clinician places an order, the system flags that PA is required, staff submit documentation to the insurer, the insurer reviews it and either approves, denies, or requests additional information. If additional information is requested, the clock effectively resets. If denied, an appeal can be filed. That appeal may go through reconsideration, an internal review, or an external independent review, in that order. PA is distinct from related terms that often get conflated. Precertification refers specifically to pre-approval for planned procedures. Step therapy requires patients to try and fail on a less expensive medication before the preferred one is approved. Formulary restrictions simply limit which drugs are covered at all. The stated rationale from payers is cost control and clinical safety. The practical tradeoff is access delay, and when care is time-sensitive, that tradeoff is not abstract. The 7 Bottlenecks That Actually Slow Things Down Understanding where delays accumulate is the first step to addressing them. There are seven recognizable choke points in the typical PA process. The first is unclear or shifting payer criteria. Documentation requirements are not always published, and they vary by plan, by drug, and sometimes by the reviewer. A submission that would have been approved last month may be denied today because the insurer quietly updated its policy. The second is administrative back-and-forth. Missing a single diagnosis code, submitting the wrong form version, or attaching the wrong clinical note is enough to trigger a rejection that requires starting over. The third is payer response time windows. Standard PA timelines can extend to 72 hours or longer. When a payer sends a request for more information, the internal clock often resets entirely. A one-week process can stretch into two. The fourth is peer-to-peer scheduling. When a clinician needs to speak directly with a payer’s medical reviewer, that call does not happen the same day. Coordinating schedules across organizations often adds several days, if not more. The fifth is the multi-layer appeals process. Even when a denial is wrong, reversing it requires going through reconsideration, then internal appeal, then potentially external review. Each step takes time that the patient does not always have. The sixth is specialty pharmacy logistics. Even after a medication is approved, it still needs to go through benefit investigation, prior authorization at the pharmacy level, and shipping. A three-day clinical delay can become a 10-day total delay by the time the medication arrives. The seventh is re-authorization for ongoing therapies. Patients on stable chronic medications or biologics frequently have to re-qualify mid-treatment. If re-authorization is delayed, therapy is interrupted even though the clinical case has not changed. How Delays Translate Into Worse Outcomes There are six reasonably direct pathways from a PA delay to clinical harm. The first is disease progression. When a patient is waiting for approval, their condition does not pause. Inflammatory conditions flare. Tumors progress. Infections advance. Every day without treatment is a day the disease is running without resistance. The second is missed diagnostic windows. A delayed MRI or lab panel can push a diagnosis into a later and less treatable stage. The decision to image was made at the right time. The image just never happened when it should have. The third is therapy interruption. Stopping and restarting a medication is not the same as never starting it. For some treatments, consistency is the mechanism of action. Interruptions reduce efficacy and, in some cases like certain psychiatric or antiretroviral medications, increase resistance risk. The fourth is substitution with inferior options. Step therapy forces patients onto less effective treatments first. A patient who needs a biologic ends up on an NSAID. A patient who cannot tolerate a first-line medication must fail it formally before a better option is approved. The fifth is avoidable emergency department visits and hospitalizations. When outpatient care is blocked, conditions escalate. A patient who could not get a covered infusion appointment ends up in the ED. That visit is more expensive, more traumatic, and more resource-intensive than the outpatient care that was delayed. The sixth is treatment abandonment. Many patients simply stop pursuing care when the approval process becomes overwhelming. The complexity, the phone calls, the re-submissions, and the uncertainty are enough to cause some patients to give up entirely. What the Evidence Shows The professional and research consensus on this is consistent. The American Medical Association has surveyed physicians annually on PA and found, year after year, that the majority report that PA has caused delays in care, and a significant portion report it has led to serious adverse events for their patients. Studies tracking overturned denials are particularly telling. When PA denials are appealed and reversed, it means the original denial was incorrect. But the reversal does not undo the delay. A patient whose approval was held for three weeks while an appeal worked its way through review still waited three weeks. The clinical damage from that window is not recovered just because the final answer was yes.
The Real Cost of Administrative Burden on Small and Independent Clinics In 2026

The Real Cost of Administrative Burden on Small and Independent Clinics In 2026 Independent clinics are quietly bleeding out, not from malpractice or bad clinical outcomes, but from the sheer weight of running a practice in 2026. If you own or manage a small practice, you already know the feeling: you finish seeing patients, and then the real work begins. Prior authorizations, denial appeals, credentialing renewals, payer portal logins, HR questions, and billing calls from confused patients. It does not stop, and most owners have no idea how much it is actually costing them. This article breaks down the real costs of administrative burden on independent clinics, gives you a model to quantify your own exposure, and points to practical fixes that do not require an enterprise IT budget or a team of 20. What Counts as Administrative Burden (And What Does Not) Administrative burden is not just “paperwork.” For the purposes of this article, it is every non-clinical task your practice must complete to get paid, stay compliant, and keep operations running. That includes billing and claims work, denials management, prior authorization, eligibility and benefits checks, coding documentation demands, payer portal navigation, contracting, credentialing, compliance tasks, HR, scheduling friction, and patient billing calls. What it does not include is clinical documentation that genuinely improves care quality, or true patient-facing clinical coordination, though admin-heavy workflows have a habit of bleeding into both. A useful way to sort the pile: some burden is payer-driven (authorizations, portals, claim rules), some is regulation-driven (HIPAA, reporting requirements, licensing), and some is internal process-driven (manual handoffs, duplicated data entry, undefined roles). Each category needs a different solution. The Real Cost: A 5-Bucket Model to Quantify Admin Burden Most clinic owners look at payroll and software costs, add them up, and stop there. That calculation misses most of the damage. Here is a more complete model. Bucket 1 is direct labor costs. Bucket 2 is lost clinician time. Bucket 3 is revenue leakage. Bucket 4 is technology and vendor overhead. Bucket 5 is hidden human costs like burnout and turnover. Run through each one, and you will likely find your administrative burden is worth two to four times what you assumed. Bucket 1: Direct Labor Costs (The Obvious Part) In independent clinics, the front desk, biller, medical assistant, office manager, and often the owner personally carry the administrative load. Common labor-heavy workflows include eligibility checks before every visit, claim status follow-up calls, payment posting corrections, scanning and faxing referrals, and spending time inside payer portals that are each designed differently. To estimate this cost: take the hourly loaded wage for each role (salary plus benefits and employer taxes), multiply by the hours per week spent on admin tasks, and add overtime and any temp staffing you rely on during crunch periods. One pattern that makes it worse is what operations consultants call “role drift,” meaning clinical staff end up doing non-clinical admin work because the system around them is broken. When your medical assistant spends 40 minutes a day tracking down prior auth status updates, that is clinical capacity being converted into administrative overhead. Bucket 2: Lost Clinician Time (The Expensive Part) Thirty minutes per day of physician admin time feels manageable. It is not. A physician generating $250 per clinical hour who spends 30 minutes a day on non-clinical tasks loses roughly $3,000 per month in potential collections. Multiply that across a year and across two or three providers, and the number gets uncomfortable fast. Beyond the math, there is a downstream effect that compounds the problem. When physicians are squeezed on time, visits get shorter, documentation gets rushed, and coding errors increase. More coding errors lead to more denials. More denials lead to more admin work. The loop closes on itself. Bucket 3: Revenue Leakage (The Silent Killer) Revenue leakage is the money you earned but never collected. It shows up as undercoding, missed charges, timely filing misses, denied claims that no one got around to appealing, write-offs from inaccurate eligibility checks, and bad debt from patient balances that were never clearly communicated upfront. Leakage gets worse when admin is overloaded. When one person owns too many steps with too little time, follow-up cadences slip, and partial payments go uncontested. To estimate your leakage exposure, look at your denial rate multiplied by your average allowed amount, then estimate the percentage of those denials that are never recovered. Add in your A/R aging beyond your target days. For many independent clinics, that number alone justifies a full workflow review. Bucket 4: Technology and Vendor Overhead (Death by a Thousand Tools) A typical small clinic in 2026 is running some combination of an EHR, a practice management system, a clearinghouse, an eligibility tool, a prior auth tool, an eFax service, a phone system, a patient texting platform, a payment processor, a reputation management tool, compliance training software, and a security solution. That is before you count the three or four payer portals with separate logins. The cost is not just the subscription fees. It is the implementation time, the staff training, the credentialed access setup, the password resets, the duplicate data entry between systems that do not talk to each other, and the hours your office manager spends managing vendors instead of managing operations. The term for what happens when tools do not integrate is “workflow tax.” Staff become the integration layer, manually moving data from one screen to another, which is both slow and error-prone. Here is a simplified look at where tech overhead tends to cluster in independent clinics: Tool Category Avg Monthly Cost Internal Hours to Manage Integration Risk EHR / PM System $300-$1,200 8-15 hrs High if siloed Clearinghouse $100-$400 3-6 hrs Medium Prior Auth Platform $200-$600 5-10 hrs High Patient Communication $100-$300 2-4 hrs Medium Compliance / Security $150-$500 4-8 hrs Low to Medium The dollar costs are often manageable. The internal hour costs are where small clinics get hurt. Bucket 5: Hidden Costs (Burnout, Turnover, Patient Experience) The path
AI Agents vs Traditional Prior Authorization Teams: Why Clinics Are Automating Prior Authorization
Why Physicians Spend 13 Hours a Week on Prior Authorizations and What It’s Costing You Prior authorization has a way of finding you before your day even starts: it’s 7:15 AM, your first patient hasn’t walked through the door yet, and you’re already staring at a backlog of PA requests, payer portal notifications, and voicemails from pharmacy staff. By lunch, you’ve spent 45 minutes justifying a medication your patient has been stable on for two years. By end of day, you’ve done a peer-to-peer call that should have taken 10 minutes but ate into your last appointment slot. This is not an unusual Tuesday. This is most days for most physicians. According to the American Medical Association, physicians and their staff spend an average of 13 hours per week managing prior authorization requests. That number sounds manageable until you do the math: that’s over 650 hours per year, per physician, spent on administrative friction rather than patient care. This article breaks down where that time actually goes, what it’s genuinely costing your practice, and how to start clawing it back. What Prior Authorization Actually Looks Like Day to Day Prior authorization (PA) is the process by which a physician must obtain approval from a patient’s insurer before a medication, procedure, or imaging study is covered. In theory, it’s a utilization management tool. In practice, it’s a multi-step gauntlet. A typical PA workflow looks like this: a prescription or order is placed, staff checks whether the payer requires approval, a form is submitted with clinical documentation, the insurer reviews it, and then a decision comes back. Except it’s rarely that clean. Payers reject submissions for missing documentation. Portals go down. Fax numbers change. Criteria differ between the pharmacy benefit and the medical benefit for the same drug. Physicians end up pulled into tasks that feel decidedly non-clinical: rewording justification language to match payer criteria, providing medical necessity explanations for treatments they’ve ordered dozens of times, and jumping on peer-to-peer calls with insurance reviewers who may or may not have the same clinical background. The friction compounds when you’re managing multiple payers, each with their own portal, their own timelines, and their own moving target of requirements. Why 13 Hours Is Actually an Undercount The 13-hour figure captures time spent directly on prior authorization tasks. It doesn’t fully account for what researchers call “attention residue,” the cognitive cost of switching between clinical work and administrative tasks. A physician stepping out of a patient room to handle an urgent PA request doesn’t just spend 12 minutes on the call. They spend the next several minutes mentally re-entering the clinical context they left. Multiply that across a full clinic day and the real productivity loss is considerably higher than the clock suggests. PA work also bleeds into evenings and weekends. Documentation reviews, peer-to-peer prep, and appeals don’t always fit neatly between appointments. For many physicians, prior authorization is a direct contributor to burnout, not because of any single task, but because of the accumulated sense that clinical judgment is being second-guessed by systems that don’t know your patients. The Real Cost Breakdown The cost of prior authorization to your practice falls into three distinct categories. Direct labor costs Include every staff member who touches a PA request: medical assistants pulling records, nurses documenting clinical rationale, front desk staff submitting through portals, and billing staff tracking outcomes. Physician time, priced at a fully loaded hourly rate (salary, benefits, malpractice, overhead), is the most expensive input in that chain. When you calculate the true cost, use fully loaded figures rather than base salary alone. Opportunity cost Is where the numbers get uncomfortable. Every hour a physician spends on prior authorization is an hour not spent on a billable patient encounter. One peer-to-peer call can displace a short follow-up visit. Repeated PA interruptions reduce scheduling flexibility, particularly in specialties like oncology, rheumatology, and cardiology where prior authorization volume tends to run high. The formula is straightforward: hours per week multiplied by your practice’s contribution margin per visit gives you a concrete weekly figure. Downstream costs Are the hardest to quantify but arguably the most significant. When prior authorization delays run long, patients abandon treatment, develop complications from uncontrolled conditions, or simply go elsewhere. That last outcome, known as patient leakage, is both a revenue and a reputation problem. Online reviews, front desk conflict, and lost referral relationships all trace back to approval delays that felt avoidable. Where the Process Breaks Down Most PA problems are process problems masquerading as payer problems. Yes, insurers make this harder than it needs to be. But practices that struggle most with prior authorization volume often share common internal weaknesses: no clear ownership, no payer-specific documentation, and no tracking system to identify patterns. The most common bottlenecks include submitting incomplete documentation on the first pass, coding and diagnosis specificity that doesn’t meet payer criteria, and no internal escalation path when a request stalls. If your practice has a high rework rate (multiple submissions for the same request), frequent last-minute peer-to-peer calls, or approvals that arrive after the clinical window has closed, your PA process is leaking money at multiple points. Six Practical Ways to Reduce Prior Authorization Time Standardize your documentation at the point of care: Build visit note templates for your highest-PA services that automatically capture diagnosis specificity, prior therapies tried, contraindications, relevant labs, and guideline references. The goal is to make the information payers need easy to extract without the physician having to reconstruct it later. Build payer-specific playbooks: For your top five payers, document the required forms, common denial triggers, portal steps, typical turnaround times, and escalation contacts. Maintain and update these quarterly. A new staff member with a good playbook will outperform an experienced one working from memory. Create a dedicated PA triage lane: Assign ownership: one person or role that is responsible for tracking every open request, escalating stalled ones, and communicating status updates. Set internal service level agreements, same-day submission for urgent cases, 24 to 48 hours for